
The article in the New England Journal of Medicine, "Ensuring a relatable platelet supply in the United States," raises an important call to action.
The question is how.
William Riley, a professor in Arizona State University’s College of Health Solutions and a co-author of the article, said a shortage of platelet collections has caused some hospitals to delay transfusions.
ASU News talked to Riley about why the shortage is happening and what can be done to address it.
Note: The interview has been edited for clarity and brevity.
Question: When and why did this shortage begin?
Answer: It hasn’t begun recently, but it’s become more serious. For the two-year period from 2017 to 2019, platelet use increased 19%, but platelet donations decreased 2% during that same time period. Again, there’s been a platelet shortage for decades, but it’s getting worse. And the primary donors for platelets are an older age group that’s aging out, which makes it even worse.
Q: Why is platelet usage increasing?
A: The four main uses for platelets are trauma, intensive care, leukemia and other (cancers). Because the population is aging, the number of people who need that type of care is increasing.
Q: The article mentions that some hospitals are having to delay transfusions. Could go you into more detail about some of the ramifications of the shortage?
A: Surgeries are getting delayed. Therapies are delayed. Outpatient transfusions are being postponed. What’s of even greater concern is surge capacity and then a public health emergency. There’s a total consensus among experts that we do not have surge capacity or emergency response capacity. Those are really important distinctions. Surge capacity is in normal periods. But a public health emergency would be impossible to respond to with the current shortage.
Q: How did COVID-19 impact the shortage if at all?
A: It just exasperated it further. What happened during COVID is that the demand for blood products and platelets actually went down, but the donor donations went down even more. Supply went down further than demand.
Q: Is one part of the shortage due to the time it takes to give platelets compared to giving whole blood, which takes maybe 20 minutes?
A: So, 94% of platelets in this nation come from what’s called apheresis (the removal of plasma from the body by the withdrawal of blood). The problem with apheresis is it takes a lot of time, which is why the donation rate is so much lower than the 13 million units of whole blood. It takes about 90 minutes, and the people who are willing to do that and do it again and again are aging. There is technology that exists in the lab for a blood blank to collect one unit of platelets from four units of blood, but it’s very time intensive and very labor extensive. That’s why only 6% of the 2.5 million transfused platelets in this country come from that technology.
Q: The article mentions the semiautomated and fully automated processes used to collect platelets in other countries. Why haven’t they been approved in the U.S.?
A: That’s the key question. The technology is there, and it’s proven, but there are different sectors in transfusion medicine, and each of those sectors has an important role to play. It’s the manufacturers of the equipment and the supplies, it’s the blood banks that actually get donations like the Red Cross and so forth. And then it’s the hospitals that use them. All three sectors are very aware of this technology, but a request has not been made of the FDA (Food and Drug Administration), and the evidence has not been granted for the FDA to approve it. These technologies would end the shortage.
Q: So, why hasn’t a request been made of the FDA?
A: The cost of conversion is expensive. The cost of operation is less expensive than the current approach. So, these three sectors that I mentioned … what physicians want is safe, effective platelets for their patients. Blood banks have to be able to do this but make it affordable. And the suppliers will do whatever the blood banks demand. It would take capital costs for the suppliers and the blood banks to convert from the current system to one or more of those other technologies.
Q: Do you anticipate the FDA will look and possibly approve these technologies over the next few years?
A: Hopefully. It sure seems like we’ve reached a consensus of the various interests. My colleagues on this paper are highly respected and well connected in transfusion medicine. We have been working with the FDA to do preliminary groundwork. The FDA is very aware of this. We also think we’ve been able to address the needs of each of those three sectors. We’ve got the credibility and the ability to bring this forth in a way that all three of the sectors will support. We’ve been working with BARDA (Biomedical Advanced Research and Development Authority in the U.S. Department of Health and Human Services) to develop an approach. So, we do have a plan. We do have recommendations. We do have strong support from the entire industry.
Q: What’s next, then?
A: Even though the data on these technologies is available from Europe and from Canada, the FDA may still need some data that we would do. But we can do that. The first phase is to do the preliminary study, gather all the evidence and meet with the FDA. Then, if the FDA approves, they would probably identify other types of data that they need in order to move forward. That would probably take two years or so. Then, whatever studies the FDA would want to fill any gaps that there might be on the evidence, we would conduct those studies and that might take a year or, who knows, three years or so forth. After that is done, the third phase is working with the three sectors (and) the equipment manufacturers to create a cost-benefit model that shows the benefit to society, the benefit to the taxpayer and so forth would be worth the return on investment.
For those who would like to donate platelets, learn more at American Red Cross website or the Vitalant website (formerly known as United Blood Services).
Top photo from iStock.com
More Health and medicine

ASU team part of nationwide study looking at Type 2 diabetes in youth
Near the end of an interview in which he talked about the work his team will be doing to tackle the rise in Type 2 diabetes among youth, Arizona State University Professor Gabe Shaibi answered why…

Leading the way in wellness: ASU highlighted in The Princeton Review's 2025 Mental Health Services Honor Roll
Being a college student isn’t easy — navigating new routines, people and places can be a challenge, especially if the right support system is not in place. That's why Arizona State University is a…
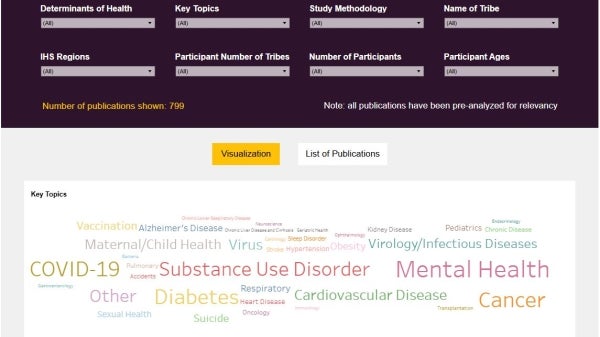
New Indigenous health dashboard offers robust database for scholars
By Nicole Greason and Kimberly Linn A team at Arizona State University’s College of Health Solutions and American Indian Studies program has created a new tool to aid researchers…